For patients and therapists;
DID stands for dissociative identity disorder.
For most people with DID, it only becomes a disorder in adult life,
but they have lived with this disorder since early childhood.
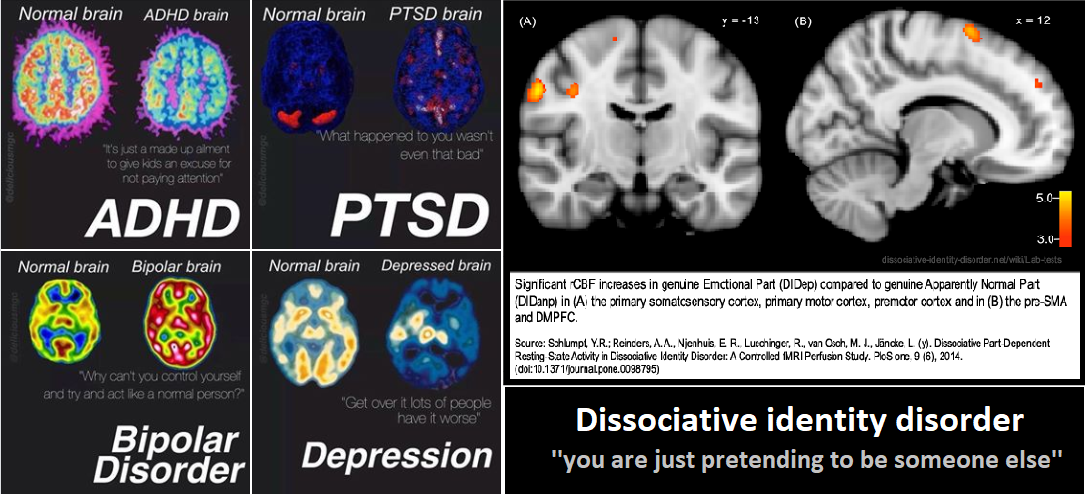
Next to DID being a disorder, it is also a remarkable coping mechanism our brain came up with in order to survive the most horrendous forms of trauma. Yes, DID is visible in the brain. It’s not fantasy based or purely based on what’s going on in the mind. There is actually a study in the links and resources tab that shows people with DID are actually pretty low on the scale of how much fantasy capability we have. We are only one step above ”mentally healthy people” and 2 steps under people who visit paranormal events.
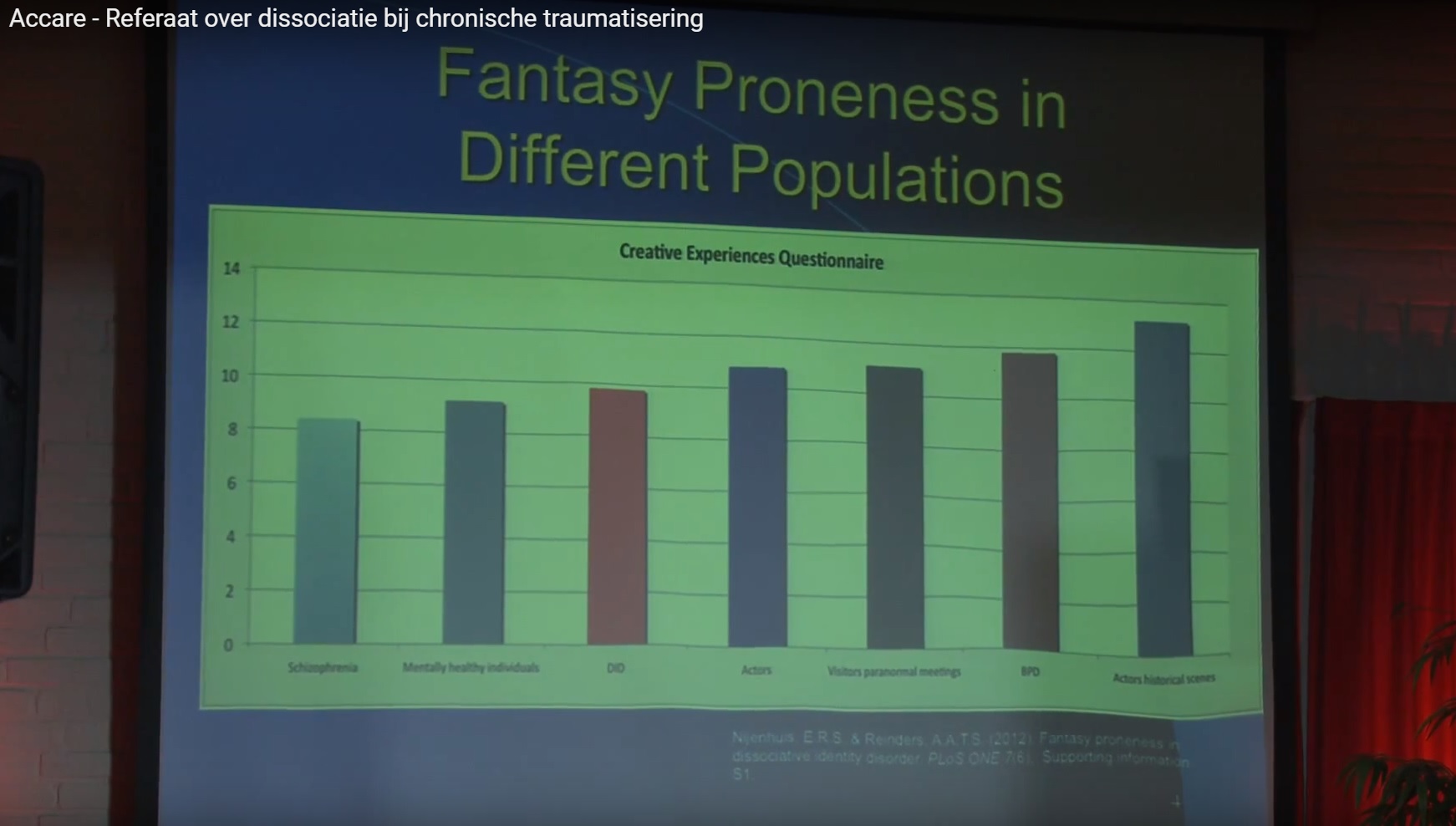
The red bar shows DID on the left side shows DID.
It’s not a personality disorder either (not since 1994 at least)
and should not be treated as one either.
I truly believe every compassionate trauma therapist can treat DID.
I also think most compassionate trauma therapists are scared to mess it up, to have boundaries broken or to have to give up halfway themselves because they can not deal with the amount of trauma we, the patient have suffered with. Luckily, Onno van der Hart, Kathee Steele and Suzette Boon wrote a book called treating trauma related
dissociation. Which includes a number of chapters on how to help yourself and your clients. I highly recommend this book to therapists who are willing to treat DID but don’t think they have the skills or specific knowledge needed.
I think in most cases this is not true. Especially not since there are enough current,
up to date books, article and studies on the subject available.
In the UK PODS is giving workshops all year round. We have a links and resources page available in the top menu with links to all these events. We hope to be able to keep it updated with events for both professionals and for people with DID.
Like said before, DID is only caused by extensive, repetitive childhood trauma, in which attachment plays a big role. If a child is comforted after trauma, the chance for DID is (way) less then when there is no comfort. Childhood trauma does not equal abuse.
One can also get DID from medical trauma, or even natural disaster.
Although that is more rare due to the fact that natural disasters often, hopefully,
don’t happen repetitive, without nurturing after the traumatic event before the age of 9.
Opinions and research on ”before which age should the abuse have happened”
vary from age 5 to 9. Which is related to the age in which a non traumatized child integrates its personality.
Alters/headmates can all have their own individual name, age, likes and dislikes, background stories, hobbies, fears, skills and time zone they are currently believed to be in. That sounds sci–fi but it sadly just means being stuck in the past, stuck in the trauma.
In some systems some alters need glasses while others don’t. Alters can also have different allergies or experience pain somewhere in the body whenever they are ”in it”.
Some systems are very covert. It might be impossible to notice a switch or that you are talking to someone else. While in other systems only certain alters can mask ”the front person” /host/original/core. One thing we should all agree on right from the start is that NO movie has ever represented DID scientifically correct or even appropriate. People with DID mostly hurt themselves or their alters. Not outside people.
DID is also not ”faked” more than any other disorder. People who fake DID are either not healthy people or very confused or misdiagnosed people.
If you worry you fake DID i suggest watching this video:
[youtube https://www.youtube.com/watch?v=2sJkvYWuYM8&w=560&h=315]
Both Onno van der Hart and Ellert Neijenhuis have written that it’s okay to call alters by their individual name if this is asked for by the alter. (haunted self and treating trauma related dissociation) Onno even says to never let it become a power struggle.
It’s our truth, our reality, and it has been since the day we were subconsciously created in our brain, to survive that which no one should ever have to go trough.
Many people with DID do not remember their (full) trauma’s.
And amnesia of either trauma, past, current, big life events or every day life events
(aka losing time) needs to be present in the patient to be able to be diagnosed with DID.
Other dissociative disorders do not include Amnesia.
DID (amnesia and distinct parts),
OSDD1a (amnesia and not distinct parts)
or OSDD1b (distinct parts but no amnesia)
The amnesia does not have to go for ALL alters. Some alters might have no amnesia at all. If they present in your office first, it can be hard to diagnose DID. Please know within the DID community we are educating that it is okay to tell your therapist what is wrong or actually going on. But because of shame and stigma, the many rejections by previous therapists most of us have experienced at some time in our life, we might not be able to disclose the DID to you until a later time, sometimes even years.
DID is not a rare disorder. Current statistics say 1-3% of the world population has DID.
More recent studies even say 1 in 100 has a dissociative disorder. For comparison, about 1 % of world population has schizophrenia ( an also stigmatized and often misunderstood disorder) And DID is also more common than bulimia.
Personally we think the numbers might even be higher.
Because sadly statics also shows it can easily take 6 to 8 years to get a correct diagnosis of DID even if you are self aware! It’s a disorder that comes with shame, with the fear of not being believed, traumatized people whom have always been told to never tell. So the 1-3% is based on correctly diagnosed people. Many are not diagnosed at all or incorrectly diagnosed. Luckily, or sadly, just from which perspective you look, PTSD also gets misdiagnosed in nearly 50% of the time!
Many people think that an alter/headmate/”personality” is split off.
But this is not really the case. Our traumatic brains never had the possibility
to integrate into one person in the first place. Like what happens with singletons, people who are not multiple, people who do not have a dissociative (identity) disorder.
This does not mean that there can’t be such a thing as a core/host/original alter, whom often (but not always) carries the birth name. But not every system has such an alter. This is explained by 3 (possible) factors, the first one is that the abuse started at a ”later” time in life (which is so messed up to say cause any age is horrible to experience such (childhood) trauma, let alone repetitively) Another factor can be that there was nourishment and comfort after the abuse or that the person is very good at masking other people and taught themselves this (subconsciously) as another survival mechanism. The third option can be that the person got pr*gramm*d,
which i won’t go into detail about any further in this article.
It is important to know and understand though, that even when there is a core/host/original alter, alters did not ”split off from them”
Its also important to know that Alters are not the cause of DID,
they are never the reason someone has DID, they should never be blamed for having DID, and they should all be treated as equal individuals where the strive is for a cooperative functioning system.
Recommended treatment for DID is individual talk therapy, 1-3 times a week
depending on the patients functionality, motivation and ability.
Often longer sessions of 60 to 90 minutes are needed.
All alter should be included, invited and welcomed to participate in therapy.
Many professionals including the writers of the books treating trauma related dissociation and coping with trauma related dissociation, seem to think integration of memory and alters is what to aim for. I think it’s important, that the aim is what the patient wants and desires collectively. And they wont know that until they are far along in treatment. You can fight it in session 12 or you can let thing go naturally and not freak us alters out by not correctly explaining what you mean with the term integration.
And/or the difference between integrating memories vs alters. Pick your battles and aim for trust in the very first place. I will write an more extensive article about integration later. Here i will mention that the alternative to healing DID with integration is referred to as the 3 C’s Communication, Cooperation, Co-consciousness. (having multiple alters present ”and at work” at the same time.)
I hope this article was uefull on the basics on DID 101.