Dissociative Identity Disorder (DID) 101
A Modern, Affirming Guide for Therapists and Clients
Introduction
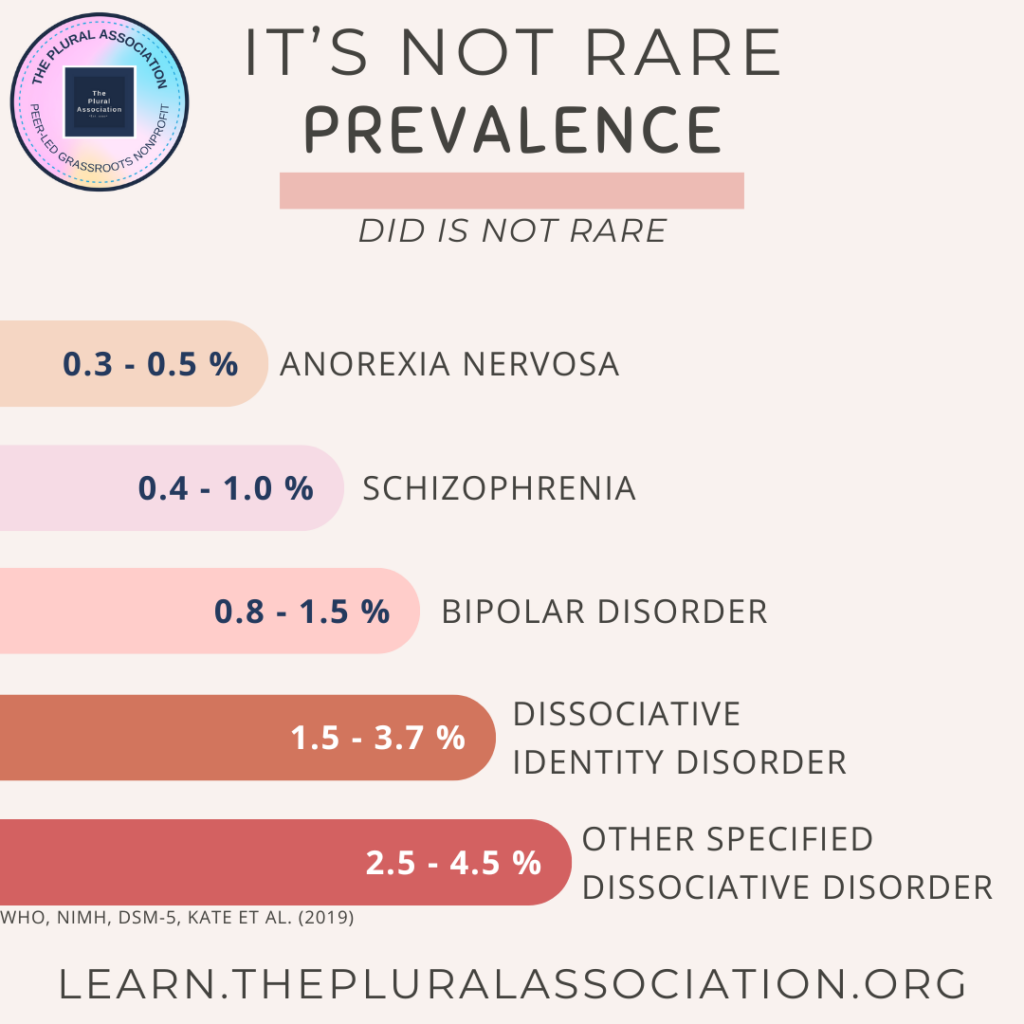
Dissociative Identity Disorder (DID) involves experiencing more than one distinct identity, consciousness, or self-state within a single body. While older clinical perspectives often presented Dissociative Identity Disorder in solely pathologizing ways, current understandings highlight that multiple identities can develop (and function) as an adaptive response to adversity—or simply as a natural expression of Plurality. DID fits under a Plural umbrella that includes many experiences of “being more than one” in a single body.
This article offers a compassionate overview for therapists, newly diagnosed clients, and anyone exploring Dissociative Identity Disorder, OSDD, or the broader Plural experience. It draws on recent community findings (including the Plural Census 2024) and explains how these insights sparked the creation of a Plural Competence training for helping professionals.
The Plural Umbrella: Where DID Systems Fit
Plurality is an inclusive term describing multiple self-aware identities or headmates sharing one body. Not everyone under this umbrella identifies with DID, nor do all with Dissociative Identity Disorder feel connected to the broader Plural community—but there is considerable overlap. Plural experiences can arise in many ways (e.g., early trauma, neurodivergence, spiritual or cultural contexts, or intentional creation) yet converge around the same core reality: “being many.”
Dissociative Identity Disorder systems typically include dissociative amnesia, distinct identities, and often early-life adversity. Still, these individuals belong within the Plural umbrella, since the central feature is having multiple internal selves that can interact and switch “front.” Whether someone relates mostly to “a DID diagnosis” or to “a non-disordered Plural identity,” both are valid paths within a diverse community of many-minded people.
Want to learn more about Plurality?
Read the Plurality FAQ
2024 Plural Census Insights
A large-scale survey known as the Plural Census 2024 shed new light on how Plural and Dissociative Identity Disorder systems view themselves and their care:
97% prefer functional multiplicity (or “Empowered Plurality”) over forced integration.
They want tools to collaborate internally without being pressured to merge into a single identity.80% stated they would not choose to stop being plural.
Many find benefits in diverse perspectives, shared coping skills, and mutual internal support.77% experience frequent moments of joy or positivity in Plurality.
This challenges stigma-driven narratives that multiple identities are only ever a burden.60% reported setbacks in therapy due to lack of Plural competence.
Misdiagnosis or disbelief have major impacts on trust and mental health progress.40% avoid disclosing their Plurality to providers, fearing stigma or forced integration.
This can undermine effective treatment or support.53% had to educate their own therapists about Plurality.
Evidencing a need for more systematic training in mental health and social services.
Plural Competence Training
In direct response to these findings, community leaders initiated a Plural Competence training for therapists, social workers, and other providers. This program covers:
Recognizing a spectrum of Plurality (DID, OSDD, endogenic systems, etc.)
Navigating trauma work without forcing unwanted “fusion”
Building rapport with multiple headmates, respecting diverse identities within one body
Addressing unhelpful myths, biases, or pathologizing language
Creating safer spaces so clients can disclose their multiplicity without fear
By bridging educational gaps, the training helps professionals better serve Plural systems, including those with DID.
Understanding DID as an Adaptive Phenomenon
Many people with DID came to experience multiple identities as a creative survival strategy—often tied to repeated adversity or trauma in childhood. The child’s developing mind learns to compartmentalize overwhelming feelings or events into separate self-states (“headmates” or “alters”), thereby preserving some continuity and resilience. Later in adulthood, these same identities might retain unique emotional tones, skill sets, or age ranges. While past adversity can lead to struggles with memory gaps or distressing flashbacks, the multiplicity itself can also become a stable, cooperative internal community—especially when approached with affirmation and understanding.
Common Myths vs. Current Insights
“DID is a personality disorder.”
DID is classified under dissociative disorders, focusing on disruptions in identity and memory, not on consistent personality traits.“They’re just faking.”
People with DID often doubt themselves already; being disbelieved can worsen shame and isolation. Research repeatedly supports the authenticity of distinct identity states.“The only healthy goal is to become one person.”
Plural Census data show that most prefer staying multiple if it isn’t causing life-threatening problems. Modern therapy aligns with the client’s own goals, whether that’s cooperative multiplicity or, if they truly wish it, a gradual blending of identities.
Recognizing and Navigating DID
Memory Gaps (“Losing Time”)
These can be alarming or confusing, but they are a hallmark of DID. Understanding that missing hours or days may be due to another headmate having fronted can reduce shame and self-blame.Switches and Co-Consciousness
Switching can be obvious or subtle. Some identities operate behind the scenes, influencing feelings, perception, or posture without taking complete control. Others shift abruptly, with distinct mannerisms and voice.Communication Among Headmates
Therapy often focuses on fostering respectful dialogue and cooperation inside. Journals, shared calendars, or internal “meeting spaces” can help create a supportive internal environment.Impact of Stigma
Sensational portrayals in media discourage many from revealing their DID or Plurality. Safe, Plural-informed spaces can significantly alleviate this isolation.
Finding Hope, Community, and Kindness
Building an Internal Culture of Care
Navigating life as a DID system can be daunting, especially right after discovery or diagnosis. Yet many find that once headmates are acknowledged and respected, a new sense of hope emerges from within. Each identity brings unique strengths—creativity, problem-solving, empathy, or resilience—and learning to share these collectively can transform a system’s daily life.
Reaching Out Beyond the System
In addition to self-awareness and trauma-informed therapy, connecting with Plural-friendly communities fosters a sense of belonging and shared understanding. Whether it’s an online forum or a local support group, hearing the stories of others who navigate life with more than one identity can bring comfort and reduce stigma’s isolating effects.
Peer Support: Many DID or Plural-led communities provide validated experience, practical tips, and moral support.
Professional Allies: Look for therapists, social workers, or coaches who recognize Plural Competence principles. They’re more likely to handle memory gaps, switching, or triggers with skill and empathy.
Self-Compassion: For newly diagnosed or newly self-aware systems, kindness toward yourself—yourselves—goes a long way. Each headmate might have different fears. Acknowledge them, comfort them, and remember you are worthy of patience.
Encouraging Connection and Hope
Even in moments of fear or hopelessness, small steps—like journaling together, reaching out to supportive peers, or locating an affirming clinician—can yield profound change. Over time, DID systems often discover they’re not alone, not “crazy,” and certainly not beyond help. Many find a renewed appreciation for the ways their identities can team up to heal old wounds, support daily functioning, and offer mutual comfort.

Approaches to Therapy and Support
Though older models emphasized merging every identity into one, modern practice highlights various goals:
Empowered Plurality
Systems learn to collaborate internally, share tasks and resources, and manage triggers while preserving distinct identities.Trauma Processing
With consent, therapy may address underlying adversities. This might include working through memories so that each headmate can hold less distress.Client-Led Goals
A system may opt for partial or full integration—or not integrate at all. Whatever the preference, person-centered care fosters trust and emotional safety.
Plural Competence training equips clinicians to uphold these client-led approaches, minimizing the harm of outdated or dismissive treatment.
Practical Tips for Clinicians and Allies
Affirm the Language They Use
Ask how a system refers to its members—“alters,” “headmates,” “people,” etc.—and adopt those terms.Respect Multiple Perspectives
Individuals in the system may hold distinct opinions or memories. Honor each vantage point and use appropriate names and pronouns.Ask About Goals
Not everyone wants to unify into one identity. Let the system set its objectives, whether that’s trauma processing, daily functioning, or building internal communication.Stay Informed
Seek resources—like the Plural Competence training—to remain updated on best practices for DID and Plurality. Don’t rely on sensationalized media tropes.Consider Group-Style Techniques
Treat therapy like a mini-group session, encouraging each identity’s input. This approach often increases internal cooperation.
Final Thoughts
Dissociative Identity Disorder (DID) can create real challenges around memory, identity, and emotional regulation. But it also rests on a foundation of resilience—the mind’s ability to protect itself under extreme stress. The Plural Census 2024 underscores how many DID systems thrive once they receive proper understanding, community support, and therapies aligned with their own goals.
Whether you’re newly diagnosed or a clinician encountering DID for the first time, remember that forced singularity isn’t the only—or even best—path. Many individuals living with DID experience a richer, more stable life through supportive, flexible care and peer communities. By embracing Plural Competence, validating the personhood of each headmate, and fostering an environment of kindness and hope, we can create a world where DID systems aren’t just surviving, but actively flourishing under the Plural umbrella.

As always, we encourage you and your System to follow your own truth, to soul search, to find words, labels, visions, theories and communities that aren’t only within your values but also match your lived experience and/or long term goals, so that you might find belonging and don’t have to try to fit in.
Thank you for investing the time to read this article. Please, feel free to leave comments or feedback in the comment section.
About the authors
The Stronghold System are the proud volunteer founders & CEO of The Plural Association Nonprofit. They are from the Netherlands and reside in a 30-something-year-old body, are nonbinary, parents of an amazing child & 3 cats. They got diagnosed with Dissociative Identity Disorder over 10 years ago & also self ID as Plural.
- Stronghold
- Stronghold
- Stronghold
- Stronghold
- Stronghold
- Stronghold
- Stronghold
- Stronghold
- Stronghold
- Stronghold
- Stronghold
- Stronghold
- Stronghold
- Stronghold
- Stronghold
- Stronghold
- Stronghold